


















































In thoracic osteochondrosis, the organs associated with the areas of the spinal cord, located at and below the affected thoracic region, often suffer. Violation of normal spinal activity leads to immobility of the arms, legs, and trunk as a whole, dysfunction of the pelvic organs, respiratory muscles, and internal organs.
Osteochondrosis is a degenerative-dystrophic disease of the spine that is based on changes in the intervertebral discs and is involved in the pathological process of adjacent vertebrae and intervertebral joints with the entire ligament.
Characteristics of the anatomy of the spine
The mobility and stability, flexibility, and elasticity of the spinal cord are highly dependent on intervertebral discs, which are a type of cartilaginous connection between bones and provide a strong bond between the bodies of adjacent vertebrae. The total length of the intervertebral discs is a quarter of the length of the spinal column.
The most important function of cartilage discs is to reduce the vertical load on the vertebrae. The disc consists of three parts:
- hyaline plates (closely adjacent to the vertebrae);
- nucleus pulposus (fills the gap between the plates);
- fibrous ring (surrounds the nucleus from the outside).
The nucleus contains cartilage cells, closely intertwined collagen fibers and chondrins (proteoglycans). The anterior surface of the cartilage discs is covered by an anterior longitudinal ligament that is tightly connected to the vertebrae and tilts freely over the cartilage discs. The posterior longitudinal strip is firmly fused to the surface of the disc and forms the anterior wall of the spinal canal. The intervertebral disc does not have its own blood supply, so it feeds on substances coming from the vertebral bodies by diffusion.
The distribution of vertical loads in the spinal column occurs due to the elastic properties of the cartilage discs. The pressure expands the nucleus pulposus and redistributes the pressure in the annulus fibrosus and hyaline plates. As it moves, the core moves in the opposite direction: when bending - towards the convexity, when bending - forward. As the spine moves, the muscles, ligaments, and discs are also involved in the work. Therefore, violation of one link leads to violation of the entire kinetic chain.
Causes and mechanisms of the disease
The mechanical effect on the spine plays a special role in the development of osteochondrosis. Under unfavorable static and dynamic loads, the nucleus pulposus gradually loses its elastic properties (due to the depolymerization of polysaccharides), forming protrusions and sequesters.
The process of disc degeneration is influenced by a genetic predisposition that causes changes in the neuromuscular apparatus of the back, changes in the structure of glycosamines, and disruption of the distribution of collagen fibers in the disc. The genetic factor is most important in the occurrence of thoracic osteochondrosis with increased functional activity.
Risk factors for the development of degenerative lesions of the spine include the anatomical features of the discs, which are imperfections in evolution. One such characteristic is the nutritional characteristics of the structures. In the human body, the plate is composed of poorly perfused tissues. Occlusion of blood vessels occurs as early as childhood. It occurs due to the diffusion of substances through the endplates after feeding.
The stimulant for nutrient entry is a dosed load that eliminates static postures and high stress. Physical inactivity is one of the leading risk factors for thoracic osteochondrosis. Therefore, regular exercise is an important preventative measure.
The peculiarity of the microscopic structure — some cells — reduces the intensity of the regenerative capacity of the plate components and the rate of recovery. Anatomical features are the weakness and lack of strength of the discs in the posterior sections. This contributes to the appearance of wedge-shaped plates in the lower chest and lumbar regions.
Involution changes are considered to be of great importance in the development of osteochondrosis. Actively degenerative changes begin to increase after 30 years. The synthesis of the components required for the disk (glycosaminoglycans) continues, but their quality deteriorates. Hydrophilicity decreases, fibrosis increases, and sclerosis appears.
Stages of degeneration of intervertebral discs:
- prolonged asymptomatic course, degenerative changes in intradiscular components, displacement of the nucleus within the disc;
- pronounced radicular symptoms of thoracic osteochondrosis, spinal cord compression, protrusion of the nucleus pulposus (protrusion, 1 degree);
- disc rupture with hernia protrusion (hernia, grade 2);
- degenerative changes in extradiscal components (grade 3).
The abnormal protrusion at various levels (neck, chest, lumbar) compresses the nerve roots, blood vessels, or spinal cord, which determines the clinical picture.
Restriction of thoracic spine mobility, which occurs due to the presence of the chest, contributes to the slightest trauma to the intervertebral discs and thus to osteochondrosis. Physiological thoracic kyphosis contributes to the redistribution of weight from the upper half of the body to the lateral and anterior sections of the vertebrae. Therefore, intervertebral hernias and osteophytes are formed on the anterior and lateral surfaces of the spine. Posterior osteophytes and hernias are extremely rare.
Osteochondrosis contributes to the narrowing of the intervertebral openings and the compression of the roots of the spinal cord and sympathetic fibers. The sympathetic fibers come from the gray matter of the spinal cord and then gather into nodes from where they reach all the internal organs. This leads to the fact that, in addition to the typical neurological disorders, thoracic osteochondrosis leads to dysfunction of the internal organs (vegetative, vasomotor, trophic) and imitation of somatic diseases. This feature of osteochondrosis of the chest plates explains the difficulty of diagnosing and prescribing appropriate treatment.
Symptoms of chest osteochondrosis
Chest osteochondrosis is more common in people who have a sedentary lifestyle. However, the applied loads have no stimulatory effect on the spine, which contributes to disrupting the recovery of the plate. Diseases develop in people who work on a computer for a long time, hunch, and so on. such people must perform therapeutic exercises on their own.
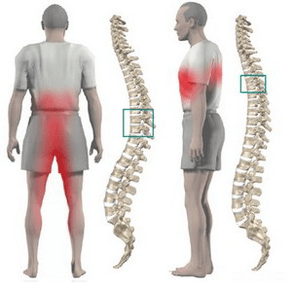
Chest osteochondrosis is most commonly accompanied by dull pain, less commonly pain and burns. The pain is localized between the shoulder blades. The patient is disturbed by a feeling of chest tightness. Upon palpation of the thoracic processes in the thoracic vertebrae, local pain is observed, which is exacerbated by axial loads reaching the spine, deep inhalation, and body twists.
Many patients have sharp pain in the shoulder blade and lower chest (posterior costal syndrome). This symptom is caused by the movement of the lower ribs. The pain increases sharply when the torso is rotated. More often than not, the pain syndrome suddenly disappears.
Often, chest pain becomes a belt that corresponds to the course of the intercostal nerve. In the innervation zone of the appropriate nerve ending, sensitivity is confused, paresthesias appear, and superficial and deep sensitivity often decreases. Possible violation of the function of the abdominal press, changes in the knee and calcaneal tendon reflexes.
Impairment of internal organs occurs when any nerve root is compressed at the 1–12 chest level. There are structures in the chest region that are responsible for innervating the lungs, heart, intestines, liver, pancreas, and kidneys. Therefore, there are no signs of chest osteochondrosis alone.
The disease manifests itself in symptoms characteristic of another pathology:
- difficulty breathing;
- intense nocturnal pain;
- "heart", angina pain;
- pain in the mammary glands;
- pain in the right or left hypochondria (symptoms of cholecystitis and inflammation of the pancreas);
- pain in the throat and esophagus;
- pain in the epigastrium, abdomen (symptoms of gastritis, enteritis and colitis);
- sexual dysfunction.
Diagnostics
The greatest value in the diagnosis of chest osteochondrosis is a chest x-ray. The picture shows the decrease in the height of the intervertebral disc, the sclerosis of the endplates, and the formation of osteophytes.
Computed tomography allows the condition of the vertebrae, the joints of the spine, the size of the spinal canal to be clarified, and the protrusion and size of the hernia to be determined.
During the differential diagnosis, a careful history should be collected and all clinical signs of thoracic osteochondrosis should be compared with those of other diseases. For example, osteochondrosis heart pain is not relieved by nitroglycerin, epigastric pain is not associated with food intake, is not seasonal, all symptoms occur mainly in the evening, and disappear completely after an overnight rest.
How to treat chest osteochondrosis?
Treatment of osteochondrosis of the thoracic spine is conservative in almost all cases. The indication for therapy is the predominance of visceral syndromes with neurological disorders. The main orthopedic treatment should be proper traction of the spine:
- active vertical traction under water;
- passive horizontal traction in a sloping bed using a Glisson loop at the level of 1-4 thoracic vertebrae in case of injury, with axillary straps at the level of 4-12 thoracic vertebrae in case of injury.
Medication consists of performing paravertebral blockages with a solution of novocaine. Painkillers and sedatives are used as the disease worsens. Ointments containing painkillers and anti-inflammatory drugs may be used at home in patients with unspecified pain syndrome.
After the acute phenomena have been eliminated, a massage of the muscles of the back and lower limbs is applied. Manual therapy is recommended for the development of functional blockages in 1-3 degree osteochondrosis. It contains various options for soft and rough effects on the back muscles.
Therapeutic practice allows for a dosed load on all parts of the spine, which stimulates recovery processes. An important condition for practicing osteochondrosis is the exclusion of vertical loads.
Physiotherapy: UHF treatment, ultrasound, inductothermia, radon and pine-conifer salt bath. Underwater traction and hydromassage are actively used in the spa section.
Surgical treatment is rarely used. The indication for surgery is compression of the spinal cord by a fragment of a dislocated disc.